Based on a post over at History Hoydens which turned into a post here, someone mentioned their favorite word was now "imperforate". danah boyd named her blog after her favorite word, "apophenia".
You would think that my favorite word would be "phoom" which does not exist in a regular dictionary, but is well-defined in the Urban Dictionary. But it's not my favorite.
My favorite word is "contraindicate". I was introduce to this term by a former housemate, Chris, who was an English major with a Latin minor when we both worked at Logitech's Tech Support. We used it when a first tier support person would be on the verge of recommending a customer reinstall windows because their mouse wouldn't work. "That would be contraindicated." we would say which would confuse them just enough to actually hear a different approach. It was also a nice way for us to say, "that's really stupid" without being lectured to by our managers.
I need to start using it. It's very handy in situations that start off with someone saying, "Hey guys, check this out...." I can stand there with my gin and tonic in hand and say, "Attempting to catch an arrow after drinking a case of PBR would be contraindicated."
After reading "The Life and Works of Guilhelmus Fabricius Hildanus (1560–1634)" Parts one and two, I have a new word to add to my list of favorites: "exarticulate". Not the definition involving one-jointed insect legs, but the one meaning to remove at the joint.
Many people balk at the thought of an amputation without anesthesia, but I know that surgeons of the 16th/17thC worked hard to reduce the pain involved mainly by applying enough pressure to stop blood and pinch nerve (providing some local anesthetic effect) and working as quickly as they could. However, the idea of a 16thC surgeon taking the time to separate the connecting tissue around the bones in the wrist or a knee is new to me. To have that procedure summed up in one word is even better: ex-ar-tic-u-late.
Sadly, the Oxford English Dictionary shows it being written first in 1658 so I can't use it prior to that. But I still can't wait to teach this some seventh graders the next time I present in a middle school.
Thursday, October 26, 2006
Not a good start
The other day, I was about to begin writing requirements for a project I've wanted to do for some time. It's a special Welcome Wagon project for the online communty of parents I help foster over at SchwabLearning.org. The idea is to alert special volunteers when someone has posted to our board for the very first time who will then be sure no newbie is left behind.
I often start documents by taking previous ones and ripping out the writing, retitling it and then start the work I need. It helps keep my documentaiton format consistent. My initial requirements docs answer these simple questions before we start working on the design: what is the problem, who is impacted by the problem, what's the solution and are there any pitfalls? Well, I grabbed a document about email subscriptions and started tearing it out to leave just the structure.
Then I looked at it again:
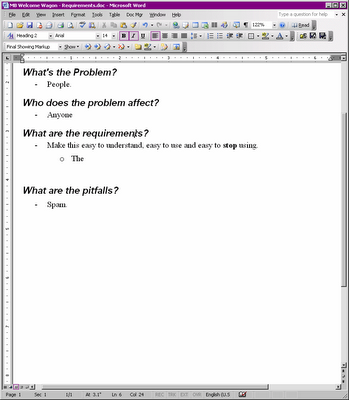
I'm going to Community Manager Hell.
I often start documents by taking previous ones and ripping out the writing, retitling it and then start the work I need. It helps keep my documentaiton format consistent. My initial requirements docs answer these simple questions before we start working on the design: what is the problem, who is impacted by the problem, what's the solution and are there any pitfalls? Well, I grabbed a document about email subscriptions and started tearing it out to leave just the structure.
Then I looked at it again:
I'm going to Community Manager Hell.
Sunday, October 15, 2006
A Woefully Incomplete History of the Treatment of Imperforate Hymen
Here's something that definitely makes my head go phoom. My friend Kalen Hughes at History Hoydens, a blog by historical romance writers, wrote me asking if I knew how an imperforate hymen might have been treated within the last, oh, 500 years. It seems this came up in the comment on her post about how "first time" sex scenes in romance novels often have the guy well past where the hymen actually is before ramming into it like a runaway train.
So here comes the first bit of explanation. I haven't blogged about this, but my hobby is reading up on the history of medicine, specifically, the history of surgery. Even more specifically, the history of surgery, the techniques and social status of surgeons, in 16thC Germany. Someday, I will blog about how I got into this and why I find it interesting. When there is some weird question about how the body and it's various bits were viewed in the past, friends quiz me.
And as they have already learned and you will soon learn, I am not freaked out by any subject. I'll get my warning out of the way now. I will be linking to sites and photographs that feature vaginas because I honestly hate typing and if I can show you a picture of an imperforate hymen, then I will (and I will).
Before we delve into how past surgeons or doctors might have viewed or dealt with imperforate hymens, it's important to demystify the hymen and then clarify what we know now about imperforate hymens.
If you really don't know what a hymen is, just start at the wikipedia entry on hymen. If you think, "I don't need no stinkin' wikipedia", that's fine. The important points here are:
Focusing on the imperforate hymen. Here are some quick notes from that emedicine.com article:
So now we know *way* more about imperforate hymens than we wanted to know. Let's see what we can find historically. Not as much as I might have hoped.
The 1901 edition of Anomalies and Curiosities of Medicine by George M. Gould and Walter L. Pyle there is a fair amount of discussion of cases where pregnancy occurred despite the fact that the hymen was not ruptured. Additionally, there are examples of women who gave birth without rupturing the hymen. There are also examples of hymen so ridged they do not allow penetration, and needed to be removed during labor in order to prevent it from obstructing the birth. Imperforate hymen is mentioned twice:
The second case fits the cases of outflow obstructions, but the first case where she became pregnant is pretty wild. Something I did not find in the modern medical literature I read so far is if the hymen membrane is porous to sperm. If anyone finds something relating to this, I'd like to know. It's not enough to assume that just because an imperforate hymen can block mucous and menstrual blood that it can block semen.
Hitting up PubMed, I came across an survey of 19thC adolescent gynecology that lists in it's abstract: "A review article in 1891 reported a 10% mortality rate associated with treatment of the imperforate hymen." (The early historical roots of pediatric and adolescent gynecology. Yordan EE, Yordan RA. Journal of pediatric and adolescent gynecology. 1997 Nov;10(4):183-91.)
Hang on a sec. There were enough instances of imperforate hymen prior to 1891 that someone could estimate a mortality rate? I will want a copy of this full article so I can read that 1891 report to see under what circumstances the surgery on the imperforate hymen was performed. (Ignore the fact that I am more curious about the possible rate of incidence than I am about mortality -- I'm used to reading about the 16thC when you were lucky if a procedure had a 50% mortality rate). I'm curious to know how many cases, what age the girls were when treated and if there are any hints about the complications that might have caused death.
Unfortunately, after this, the trail grows cold for me. Obstetrics and gynecology are not areas where I have chosen to buy books so I need some encouragement to keep researching this.
Thinking it through (often unwise without actual documentation)....
Gould and Pyle make references to stories of hymens that prevented actual coital penetration (and yet pregnancy occurred) back to the 16th and early 17thC (citing Fabricius Hildanus and William Harvey among many others). Also, it seems that depending on the nature of the hymen at the time of labor, it would either rupture during labor or it would need to be cut if it was too "fibrous" (thick and inelastic).
Knowing that surgeons of the early modern period did not hesitate to apply the knife, especially if what they were facing was not typical or ideal, I'll hypothesize that faced with an imperforate hymen, especially when it is blocking menstrual flow or obstructing a normal birth the surgeon or midwife would have simply cut it with a knife. What I cannot guess at is how much they would have cut (a single slit or circumscribe the opening) or what, if any, after care would have followed and how that might have changed with the increased understanding of circulation (William Harvey, 1628) and staunching post-partum hemmoraging.
If anyone has resources or is willing to add to the research on this topic, please add a comment. I find these specific questions interesting because they require taking into consideration societies view of the body, common medical knowledge at the moment and learning what we really know about the condition.
So here comes the first bit of explanation. I haven't blogged about this, but my hobby is reading up on the history of medicine, specifically, the history of surgery. Even more specifically, the history of surgery, the techniques and social status of surgeons, in 16thC Germany. Someday, I will blog about how I got into this and why I find it interesting. When there is some weird question about how the body and it's various bits were viewed in the past, friends quiz me.
And as they have already learned and you will soon learn, I am not freaked out by any subject. I'll get my warning out of the way now. I will be linking to sites and photographs that feature vaginas because I honestly hate typing and if I can show you a picture of an imperforate hymen, then I will (and I will).
Before we delve into how past surgeons or doctors might have viewed or dealt with imperforate hymens, it's important to demystify the hymen and then clarify what we know now about imperforate hymens.
If you really don't know what a hymen is, just start at the wikipedia entry on hymen. If you think, "I don't need no stinkin' wikipedia", that's fine. The important points here are:
- The hymen is *outside* the vagina. (And if that's news, they you *do* need the stinkin' wikipedia article.)
- There is a wide range of configurations (see Illustrations of the hymen in various states), thickness and elasticity. Generally, the hymen becomes thin and elastic with the onset of puberty so there's no tearing or blood during sex, but that's not always so.
- Because the hymen varies in how much of the vaginal opening it covers and because it is elastic, it's impossible to define what an intact hymen is and so the condition of a hymen is *not* a good indicator of virginity. (Further down, I'll point out some historical cases of women becoming pregnant despite their hymens being "unruptured".)
- In some women, the hymen does completely cover the vaginal opening. This is known as "imperforate hymen". And contrary to wikipedia's authoritative "1 in 2000" occurrence, according to the emedicine.com article on the "imperforate hymen", the occurrence has been reported from 1 in 1000 to 1 in 10000.
Focusing on the imperforate hymen. Here are some quick notes from that emedicine.com article:
- "Variations in hymenal anatomy commonly escape diagnosis until the time of menarche". So, even our modern medicos have trouble diagnosing this until a girl has her first period. (In some cases, mucous secretions will collect at birth and cause the imperforate hymen to bulge aiding in identification.
- Even if an imperforate hymen is detected at birth and unless there is an immediate problem, it's recommended to wait until puberty when the onset of estrogen will help prevent scaring of the tissue when it is surgically cut.
- When a girl with an imperforate hymen reaches menarche, the menstrual flow will have no where to go. This will cause the hymen to bulge and look bluish. If it goes untreated (it's not an emergency situation), her symptoms will include cyclic lower abdominal pain, menstrual like cramps, pressure on the bladder and rectum. If it remains untreated, her abdomen might also bulge. (See also the emedicine article on Outflow Obstructions and, as promised, pictures). This can go so far as to block the urinary tract and overflow the bladder (which will cause more abdominal pain, pressure on the rectum and vomiting). In the worst cases, fluids can build up and organs can rupture. (See Imperforate hymen as a cause of bladder perforation and intestinal obstruction.)
So now we know *way* more about imperforate hymens than we wanted to know. Let's see what we can find historically. Not as much as I might have hoped.
The 1901 edition of Anomalies and Curiosities of Medicine by George M. Gould and Walter L. Pyle there is a fair amount of discussion of cases where pregnancy occurred despite the fact that the hymen was not ruptured. Additionally, there are examples of women who gave birth without rupturing the hymen. There are also examples of hymen so ridged they do not allow penetration, and needed to be removed during labor in order to prevent it from obstructing the birth. Imperforate hymen is mentioned twice:
H. Grey Edwards has seen a case of imperforate hymen which had to be torn through in labor; yet one single act of copulation, even with this obstacle to entrance, sufficed to impregnate.( CHAPTER 1. GENETIC ANOMALIES.
Foucard 15.111 reports a case of retention of urine in a young girl of nineteen, due to accumulation of the menstrual fluid behind an imperforate hymen. (CHAPTER 15. ANOMALOUS TYPES AND INSTANCES OF DISEASE.
The second case fits the cases of outflow obstructions, but the first case where she became pregnant is pretty wild. Something I did not find in the modern medical literature I read so far is if the hymen membrane is porous to sperm. If anyone finds something relating to this, I'd like to know. It's not enough to assume that just because an imperforate hymen can block mucous and menstrual blood that it can block semen.
Hitting up PubMed, I came across an survey of 19thC adolescent gynecology that lists in it's abstract: "A review article in 1891 reported a 10% mortality rate associated with treatment of the imperforate hymen." (The early historical roots of pediatric and adolescent gynecology. Yordan EE, Yordan RA. Journal of pediatric and adolescent gynecology. 1997 Nov;10(4):183-91.)
Hang on a sec. There were enough instances of imperforate hymen prior to 1891 that someone could estimate a mortality rate? I will want a copy of this full article so I can read that 1891 report to see under what circumstances the surgery on the imperforate hymen was performed. (Ignore the fact that I am more curious about the possible rate of incidence than I am about mortality -- I'm used to reading about the 16thC when you were lucky if a procedure had a 50% mortality rate). I'm curious to know how many cases, what age the girls were when treated and if there are any hints about the complications that might have caused death.
Unfortunately, after this, the trail grows cold for me. Obstetrics and gynecology are not areas where I have chosen to buy books so I need some encouragement to keep researching this.
Thinking it through (often unwise without actual documentation)....
Gould and Pyle make references to stories of hymens that prevented actual coital penetration (and yet pregnancy occurred) back to the 16th and early 17thC (citing Fabricius Hildanus and William Harvey among many others). Also, it seems that depending on the nature of the hymen at the time of labor, it would either rupture during labor or it would need to be cut if it was too "fibrous" (thick and inelastic).
Knowing that surgeons of the early modern period did not hesitate to apply the knife, especially if what they were facing was not typical or ideal, I'll hypothesize that faced with an imperforate hymen, especially when it is blocking menstrual flow or obstructing a normal birth the surgeon or midwife would have simply cut it with a knife. What I cannot guess at is how much they would have cut (a single slit or circumscribe the opening) or what, if any, after care would have followed and how that might have changed with the increased understanding of circulation (William Harvey, 1628) and staunching post-partum hemmoraging.
If anyone has resources or is willing to add to the research on this topic, please add a comment. I find these specific questions interesting because they require taking into consideration societies view of the body, common medical knowledge at the moment and learning what we really know about the condition.
Subscribe to:
Posts (Atom)

